BRONCHIAL ASTHMA.
DEFINITION:
Paroxysmal wheeze and breathlessness occurring on account
of narrowing of airways.
In essence –hyper reactive airways- where in inflammatory
reaction involves all the 3 layers producing
1.
bronchial
smooth muscle spasm
2.
Mucosal swelling
3.
Viscous bronchial secretions
All 3 factors thus causing
narrowing of airway.
Note:
Asthma is a reversible condition (COPDand Chronic
bronchitis-irreversible)
Asthma affects
bronchi mainly(emphasyma-alveoli)
CLASSIFICATION:
According to severity,etiology,according to type of
airflow obstruction
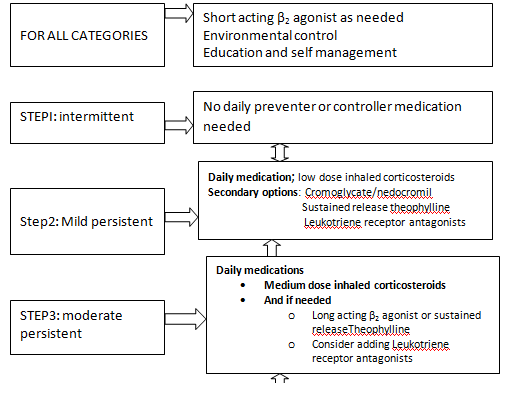
As per severity:
Intermittent less than once a week
Mild persistent .once per week/less than
once per day
Moderately persistent daily
Severe persistent daily
·
A spectrum of severity is presented in asthma
rather than a discrete severity group.
·
If grading is difficult consider the most likely
group and start treatment appropriate
for that,
-monitor by PEF and reassess.
·
Also severity can vary with time.
CLINICAL FEATURES:
Narrowing of airways causes the classic symptoms wheeze,
cough, breathlessness
Cough is especially nocturnal and dry
Attacks can be
episodic or chronic (overlap can occur)
Generally episodic
in atopic individuals –
In non
atopic-chronic asthma
Asthmatic attacks can manifest in 2 clinical forms severity wise.
·
Acute asthmatic exacerbation
·
Steady chronic
asthma
In Steady state:
Asthma starts episodically initially, becomes continuous
later, with
-symptoms of nocturnal cough, exertional dyspnoea ,tightness in the chest
-can steadily worsen and lead to acute exacerbation
Acute severe
asthma: features
Dyspnea even at rest
Patient confused/drowsy/agitated
cyanosed
Accessory muscles of respiration functioning
Respiratory rate.>30per min
Pulse rate.160/min
Inability to talk full sentences
PaO2 less than 60%; PaCO more than45%
Age group
Childhood asthma
Adult onset asthma
But can start at any age, in different situations
Clinical variants
of Asthma (Following have to be looked into for optimal management)
·
Cough
variant asthma
Cough is the sole manifestation
Persistent cough-specially
manifest in children
For Relief-Anti asthmatics
after investigations
·
Nocturnal
asthma
Definition criteria-
Overnight fall in FEV1 by
>20%or of Peek Expiratory flow rate( PEFR )
Causes of
nocturnal nature
(
Air way sensitivity at night increases 8
fold, Airway cooling at night, Plasma concentration of cortisol and adrenalin
fall at early morning. GERD reflux and
aspiration)
·
Gastric asthma
Gastro esophageal reflux worsens
asthma after meals /
Symptoms occurring only after
meal suggest GERD
·
Aspirin
sensitive asthma
Asthma, nasal polyp and aspirin
sensitivity constitute “Samptars triad”
As a general rule avoids aspirin
and NSAIDs in asthma; paracetamol may be used.
·
Exercise
induced Asthma
This feature can be sole
manifestation –treat with bronchodilators Short acting β2 agonists
And
with sodium Cromoglycate- before exercise
Triggers” (allergens)which worsen the symptoms
are-
Exercise, cold, chemicals pollen, air pollution, animal
dandruff, viral infections,strong emotions
These triggers
cause bronchial hypersensitivity through vagal nerve and Beta adrenergic
receptors
-in the airways.
Certain existing
diseases can worsen asthma and are to be looked for:
Sinusitis,
Thyrotoxicosis,
Hypertension (antihypertensive like beta blockers and ACE
inhibitors worsen asthma)
HISTORY, CLINICAL
PICTURE
Presence of following warrant the diagnosis of asthma:
·
History:
·
H/o atopy
I.e. h/o allergic rhinitis,
atopic dermatitis, eczema, or utricaria
·
Wheeze and dyspnoea which are episodic and
become continuous later.
·
Unexplained cough; viscid sputum may accompany.
·
Past h/o eosinophilia, asthmatic bronchitis, or
allergic bronchitis
DIAGNOSIS
Diagnosis is essentially clinical
·
-Chronic recurrent or persistent wheeze which
responds to bronchodilators
·
Cough may or may not be present(except in cough
variant asthma)
·
Supporting Features in diagnosis;
·
Family h/o atopy, asthma
·
Nocturnal cough or wheeze, exercise induced wheeze
·
Seasonal variation in symptoms
Cough alone is a poor marker of
asthma except in cough variant asthma where cough alone is a symptom
Additional
diagnostic supports
Demonstrating reversible airway obstruction by measuring
PEFR or FEV1
After β2 agonist administration, PEF increases
by 20% in 10 minutes.
If the diagnosis is
uncertain- broncho provocative tests is done; but should be performed only by
specialist.
DIFFERENTIAL
DIAGNOSIS
ACUTE SEVERE
ASTHMA (Status Asthmaticus is an obsolete term)
·
Symptoms
Too breathless to speak (unable
to speak complete sentences)
·
SIGNS
Pallor, sweating, exhaustion, disorientation/unconsciousness
Pallor, sweating, exhaustion, disorientation/unconsciousness
Cyanosis, tachycardia, pulse
rate.110/min, bradycardia warrants immediate resuscitation
Tachypnea. Respiratory rate
>25/min;
Accessory muscles of respiration
working
Pulsus paradoxus
Silent chest indicates severe
airway obstruction; little air moving in and out of lung to generate rhonchi.
PEFR<40 200l="" absolute="" min="" of="" or="" p="" predicted="" value="">



Arterial blood gas-PO2
falls PCO2 rises ( after initial fall
due to hyperventilation0
·
INVESTIGATIONS
1. Normal
chest x-ray/increased vascular markings
2. Peripheral
smear showing eosinophilia
3. Spirometry
showing Low FEV1/FVC ratio
FEV1-The
amount of air forcibly expired in the first second of an FVC manoeuvre.
FVC-the
maximum amount of air forcibly expired after maximum expiration
A ratio of FEV1/FVC of less
than 80% indicates airflow obstruction.
Also if after bronchodilators
the absolute value of FEV1 increases by more than20%,it indicates
reversible airflow obstruction.
4. Peak
Expiratory Flow Rate:(PEFR)
5. PEFR
is a measure of the maximum expiratory flow rate during a forced expiration.
A miniature peak flow meter
simple ,portable and cheap hand held device is used.
Advantage; patient may be
monitored at home avoiding hospitalization. In moderate asthma.
Normal PEFR are600-800ltrs/min.
for males and 400-600ltrs /min for females.
6. EXERCISE
TEST;
After an exercise challenge,
PEFR or FEV1 falls by more than 20%.
7. Allergy
test:many with asthma have positive allergy test;but it may not be the cause of
symptoms.
Further investigations for in
-patient
8. Electrolytes-hyperkalemia
can occur due to β2 agonist, steroid or
diuretic therapy.
9. E.C.G-To
evaluate myocardial ischemia.
10. 10.Arterial
Blood Gas –in severe cases
AIM OF TREATMENT:
1.
Relieving symptoms
2.
Controlling airway inflammation so that no
attacks occur
ESSENTIAL FACTORS IN MANAGEMENT OF BRONCHIAL
ASTHMA
1.
Assessment of severity of asthma (refers to
patient symptoms between acute attacks)
2. drug therapy
For symptom relief
For symptom prevention
3.
Environmental
management-by avoiding allergens and respiratory irritants
4.
Prevention
of the following
Prevention and treatment of acute
exacerbations
Prevention of irreversible
airway changes
Mortality
5. Maintenance of the following
As far as possible maintain Lung
functions normal
Maintain activity levels at
normal state
(attend
work regularly,restful sleep/normal growth in children)
6.
Avoid adverse effects of drug (optimal use of
medication)
7.
Follow up
-and regular reevaluation for chronic cases
8.
Patient education
CLASSIFICATION OF SEVERITY OF ASTHMA
CATEGORY
|
DAY TIME SYMPTOMS
|
NIGHT TIME SYMPTOMS
|
PEF( predicted)
|
Variability of PEFRorFEV1
|
INTERMITTENT
|
≤ 2/week≤
|
≤1per month
|
≥80%
|
<20 p="">
|
MILD
|
2-4 per week
|
2-4 per month
|
≥80%
|
20-30%
|
MODERATE
|
>4perweek
|
>4 per month
|
60-80%
|
>30%
|
SEVERE
|
Continuous
|
Frequent
|
<60 p="">
|
>30%
|
|


Treatment of acute severe asthma
Initial assessment
Immediate:
Ability to speak
Vital signs
Measurement of PEF unless patient is too ill to perform PEF
Arterial blood gas analysis
TREATMENT of Acute severe Asthma
1.Oxygen
High humidified Oxygen concentration
Goal Sao2 >92%
If appropriate oxygenation is not arrived assisted ventilation
2. Inhaled brocho dilators-in high dose
Short acting β2Agonist Salbutamol (5mg/hr)
Via nebulizer or via metered dose inhaler through a space devisor
3. Inhaled anticholinergics
(Iptratropium bromide may be added )
4.Systemic corticosteroids
IV hydrcotisone200mg-if patient unable to swallow or is vomiting
Intravenous fluids
Subsequent management
IV fluids
To treat dehydration and acidosis
Normal saline+sodium bicarbonate/lactate infusion
If salbutamol induced hypokalemia is present –potassium supplements
If patient fails to improve
IV magnesium sulphate
IV Beta2 agonists
IV aminophylline
IV leukotriene receptor antagonists
Anesthetics
Mechanical ventilation
Indication
Coma
Respiratory arrest
Deteoration of ABG inspite of optimal therapy
Exhaustion,confusion,drowsiness
Monitoring of treatment
Record PEF every 15-30 min
Serum concentration of aminophyline monitoring (if used)
Rpt ABG-
If initial PaCO2 was raised
PaO2 was low or If patient deteriorates.
----------------
PHARMACOTHERAPHY
POINTS OF CLINICAL IMPORTANCE
Principles involved:
1. Since asthma is a inflammatory disease regular anti-inflammatory drugs are indicated.
2. Inhaled therapy is preferable
Inhaled β2 agonist is cheaper than syrup/tablets
3. I n occasional attacks use inhalers on an as-needed basis
4. In moderate-severe cases use anti-inflammatory drugs :inhaled steroids ,then inhaled broncho dilators
5. Acute severe asthma needs intensive care therapy
TWO BASIC CATEGORIES OF MEDICINES FOR ASTHMA
1. RELIEVERS- Relieve acute symptoms
2. PREVENTERS- prevent further attacks -anti-inflammatory
Point of clinical importance:
In mild asthma – use relievers as needed
In persistent asthma-control medicines are taken on regular basis which prevent attacks.
1. RELIEVERS-QUICK RELIEF MEDICATIONS which relieve the symptoms first
Mainly broncho Dilators and Anticholinergics
Used to relieve the symptoms by broncho dilatation-act by relaxing smooth musclesof bronchi.
A. β2 agonist-Short acting)-
usually self administered in inhalant form
(if patient is unable to use inhalant oral treatment is given)
β2 agonist provide temporary relief only-do nothing to solve the underlying problem
B. Anticholinergics.(Ipratropium bromide)
Mode of action-inhibit vagally mediated broncho constriction
Less powerful than β2 agonist and slower in action-
takes 30-60 minutes for good effect
Can be used as substitute for β2 agonist (if intolerant) or as additive
Not proved useful for long term use.
C.Methyl Xanthines (e.g.theophylline,aminophylline)
Usable in combination with inhaled steroids SR theophylline –can control nocturnal asthma
Usable as an alternative to ICS in some cases of mild persistent asthma-(ifICs not available or if oral therapy is desired by the patient);
but less effective
have less favorable side effects profile.
Used only occasionally these days.
2.PREVENTERS
(LONG TERM CONTROL MEDICATION)
Used on regular basis to prevent the attack, not for treatment during the attack
Prevent patient going for chronic asthma
Preventers are anti inflammatory drugs.
Mode of action:
The airway inflammation -the hall mark of asthma, is modified by these drugs
In asthma bronchi are not only constricted but are also inflamed ‘hyper reactive,
Irritable at slightest provocation-which is to be controlled by anti inflammatory drugs
Administration:
Preventers are used twice a day -whether or not symptoms are present
Used in all patients with persistent asthma
drugs in this group-
· Frequently used drugs
anti-inflammatory drugs corticosteroids .( Inhaled,oral or IV)
broncho dilators
· other anti-inflammatory drugs
Leukotriene antagonists
Mast cell stabilizers
2.1.INHALED CORTICOSTEROIDS (ICS)
ICS are the most effective drug for asthma
Anti inflammatory in action
- reduce the frequency of acute attacks and thus improve the quality of life
Early use of ICS prevents fixed airway obstruction occurring later.
improve lung functions,
Also relieve the symptoms in addition to preventive action
Indications
ICS is first line drug for moderate and severe Persistent asthma
In mild form indication is controversial
Dose
optimal dose-is lowest dose needed for good disease control
optimal dose-is lowest dose needed for good disease control
Dose must be individualized and titrated
Increasing the dose may not be effective always
High dose of inhaled steroids may cause systemic effects
Efficacy of ICS is improved by using spacer devices
Dry powder devices like tubohaler /accuhaler increase the drug delivery to lungs
-therefore low doses are advised in such devices
Usually administered twice daily
Names of steroids:
Prednisolone, hydrocortisone betamethasone, , beclomethasone, budesonide,
triamcinalone, -fluticasone
Although the different products of ICS vary in milligram potency, for practical purposes,
doses are measured in puffs on the inhaler.
2.2.BRONCHO DILATORS-see above
2.3.LEUKOTRIENE BLOCKERS (RECEPTOR ANTAGONISTS )
Mode of action- These inhibit the effects of leukotrienes –products of arachidonic acid
metabolism
Onset of action is rapid (within 1-3 hrs)
Indications-
Indicated in persistent asthma of all degrees.
Attenuate exercise induced asthma
Are of value in aspirin induced asthma.
May act as steroid sparing agent
Use as monotherapy in mild persistent asthma debated
Disadvantage –Churg-Strauss , a systemic vasculitis is reported
Common side effect-headache,Gi disturbance
Name-Monteleukast –10mg HS (5mg chewable tabs for children)(SINGULAIR)
Zafirleukast -20mgBID (ACCOLATE)
2.4.MAST CELL STABILISERS (CROMONES)
These are Mast cell stabilizers-prevent release of inflammatory mediators from cell granules
Sodium Cromoglycate and Nedocromil, Ketotifen
Have weak anti inflammatory effects
Useful in atopics with mild asthma
Disadvantages; high cost, requires frequent dosing, poor efficacy
Main advantage is good safety profile.
Useful In asthmatics with persistent cough if optimal dose of ICS is ineffective
Useful for the prevention of exercise induced asthma
2.5.OTHER DRUGS
· Oral Corticosteroids
Indicated in poorly controlled severe asthma
Short course of oral steroids are usually necessary in acute exacerbations
(Predinisolone1-2mg/kg/day with upper limit of 60mg /day)
Dis advantage-long term use cause systemic effects
Need for maintenance therapy if no control with high dose Inhaled steroids
Frequency-daily or alternate day steroids
in children take extra care in stress ful situation like surgery.
· ANTI IGEN ANTIBODY
Omilizumab which block the immune system pathway triggered by allergens
· Long term β2 agonist(LABA )inhalers open the airways for several hours
Salmeterol, formoterol administered twice daily since they are long acting
nocturnal symptoms are controlled by this sustained action
Prevent exercise induced asthma (provide longer protection than short acting)
Formoterol may be useful in acute asthma because of quick onset of action in 15 min.
LABA inhalers have synergistic effect with ICS (better effect than doubling dose of steroids)
Side effects-palpitations tremors
Note: Single medication that combines steroids and bronchodilators may be used.
· Anti histamines
- Have shown no proven benefit;
PATHOPHYSIOLOGY OF ASTHMA
PAthophysiology of asthma is a very complex and controversial one.
Pathophysiology forms the basis of therapeutics of asthma
Two basic entities that occur :
1. ROAD-Reversible Airway Obstruction
2. BHR-Bronchial Hyper reactivity.
--------------
---------------------------------------------------------



0 comments:
Post a Comment